Home › Forums › Sleep Dentistry › Snoring Treatable By Dental Device › Snoring Treatable By Dental Device
CONTINUOUS POSITIVE AIRWAY PRESSURE: HIGHLY SUCCESSFUL, HIGHLY REJECTED
 |
 |
|
Figure 1. Patient sleeping using continuous positive airway pressure (CPAP) therapy. |
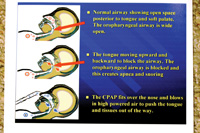
Figure 2. Diagrams show how CPAP functions. |
After weight loss, the number-one medical treatment for snoring and OSA is CPAP therapy. It is an extremely successful treatment modality for these problems. (Figure 2 shows how the CPAP device functions.)
However, CPAP therapy presents its own difficulties since it is not tolerated by 50% to 60% of the patients who are treated with it.4,5Some of these difficulties include dry/stuffy nose, irritated facial skin, sore eyes, and headaches. If the CPAP device is not properly adjusted, the patient may get stomach bloating and discomfort while wearing the mask. Without the ability to wear the CPAP device, these patients are left to “fall through the cracks” untreated. Where do they go, and what hope do they have for the successful treatment of their condition?
ORAL SLEEP APPLIANCES
 |
 |
| Figure 3. The Tap appliance, an example of a double-arch appliance that opens the bite and positions the mandible/tongue forward. |
Figure 4. The SUAD appliance, another example of a double-arch appliance. |
 |
|
Figure 5. Tongue-retaining appliance that holds the tongue forward with suction. |
The answer for people who are CPAP intolerant lies with dental sleep appliances. In the proper diagnosis and use of oral sleep appliances, dentistry has a workable solution for sleep apnea and snoring. With this, dentistry has been handed a major responsibility in the treatment of snoring and OSA.
For the most part, the dental devices currently available for the treatment of snoring and OSA are double-arched appliances. Success is achieved by opening the vertical dimension and advancing the mandible forward.6 The advancement can be from edge-to-edge to, as much as, a full protrusive position. With some patients, the vertical is opened as much as 10 to 15 mm. In this way, the tongue is pulled forward and the airway opened.
Two popular double-arched sleep appliances that advance the mandible and open vertical are illustrated in Figure 3, the Tap appliance, and Figure 4, the SUAD appliance.
Another option is the tongue-retaining device (Figure 5). It holds the tongue forward by suction, created when the tongue is inserted into a rubber bubble in the front of the appliance.
Appliances like these can be successful, however, a large percentage of them can be uncomfortable since mandibular advancement can lead to jaw pain, changes in occlusion, and tempromandibular disease problems. Furthermore, what can be done once the dentist has opened the vertical, and moved the jaw forward as far as possible, without accomplishing the reduction of snoring and apneic events? The treatment is finished, unsuccessfully.
SINGLE-ARCHED APPLIANCES
In September, 2006, a new maxillary single-arch oral sleep appliance was introduced to dentistry called the Full Breath Solution (FBS). It allows the clinician to take a very different approach to treatment. Rather than pulling the tongue forward by advancing the mandible, it works by utilizing a “tail” that restrains the tongue from moving upward and backward. The tail is expanded posteriorly and inferiorly, depressing the tongue in the same manner in which the medical doctor utilizes a wooden tongue blade in an exam. The tongue is gently depressed in order to open and view the airway. In the same way, dentists can utilize the tail on the single-arch FBS oral appliance to open the airway.
In June, 2009, the mandibular single-arch FBS oral appliance was granted FDA certification, and subsequently introduced into patient care. This was the fifth FDA certification granted to the FBS appliance since 2004.
The CPAP is almost 100% successful, when tolerated, because the positive pressure of the continuous air stream pushes the tongue forward keeping the airway open. Similarly, the FBS oral appliance is successful because it depresses and restrains the tongue, inhibiting the tongue from moving up/backward and blocking the airway. An oral device that controls the tongue is able to control and open a patient’s airway, allowing more oxygen to enter the lungs, dramatically improving nighttime breathing.
 |
 |
|
Figures 6a and 6b. Single-arch maxillary Full Breath Solution (FBS) appliance. |
 |
 |
|
Figure 7. The tail of the lower FBS which can be seen here depresses the tongue and prevents it from moving posteriorly. |
Figure 8. An underside view of a mandibular FBS appliance. Two to 4 clasps are placed for retention. |
Figures 6a and 6b show the maxillary FBS oral appliance, and Figures 7 and 8 show the mandibular FBS oral appliance. The mandibular FBS single-arched appliance utilizes a posterior tongue restrainer (PTR), or “tail” to depress the tongue.
The FBS appliance gains its clinical success by small additions of acrylic to get posterior and inferior extension of the PTR (tail). This allows for more leverage in restraining the tongue. The formation of the tail, which acts exactly like a tongue depressor, prevents the tongue from its upward and backward movement resulting in an open airway and reduced/eliminated snoring.
 |
 |
|
Figure 9. Blue wax has been added to the tail of the maxillary FBS appliance. |
Figure 10. Blue wax has been added to the tail of the mandibular FBS appliance. |
 |
 |
|
Figures 11 and 12. Wax has been removed and replaced with cold-cured acrylic to the same approximate shape both a maxillary and a mandibular FBS. The tails can now function like a tongue depressor to open the airway. |
With either the maxillary (Figure 9) or mandibular appliance (Figure 10), wax is incrementally added to the tail, a little at a time, to clinically test for patient comfort and tolerance. If comfortable, the wax is removed and acrylic is added in the same approximate size and shape as the wax-up (Figures 11 and 12). In this way, the tail is expanded (from its original lab-fabricated starting point) to adequately depress the tongue.
Depression can be slight, or much deeper, depending on the patient. The question that invariably comes up is the comfort of the tail. Approximately 5% of patients complain of discomfort or irritation. In those cases, the tail is cut off. Then, approximately 3 weeks later, the tail is added back on in small increments of acrylic extensions. This approach produces a uniform success rate with patients (breathing and comfort) in the 99th percentile. When desired, acrylic can also be removed from the superior surface of tail to keep it thinner and more comfortable.
Despite the tail, the properly fabricated and adjusted FBS appliance will not cause gagging. The reason lies with the physics and effects of snoring. When a person is snoring, the tongue falls back and closes the airway from 80% to 90%. As the air flows through the constricted airway, it picks up speed as it moves through the reduced opening. This constantly speeding air desensitizes the nerve endings on the posterior section of the tongue. As a result, there is a reduction or elimination of the normal gagging reflex due to a reduction of tactile nerve endings on the tongue.