Home › Forums › Endodontics & conservative dentistry › RADICULAR CYST
Welcome Dear Guest
To create a new topic please register on the forums. For help contact : discussdentistry@hotmail.com
- This topic has 8 replies, 4 voices, and was last updated 22/03/2012 at 5:43 pm by
 drmithila.
drmithila.
-
AuthorPosts
-
19/03/2012 at 5:57 pm #10395
 drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 times
drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 timesIntroduction:-
Radicular Cyst is the most common odontogenic cystic lesion of inflammatory origin. It is also known as Periapical Cyst, Apical Periodontal Cyst, Root End Cyst or Dental Cyst. It arises from epithelial residues in periodontal ligament as a result of inflammation. The inflammation usually follows death of dental pulp. Radicular cysts are found at root apices of involved teeth. These cysts may persists even after extraction of offending tooth, such cysts are called Residual Cysts.
Defination:-
It is defined as an odontogenic cyst of Inflammatory origin that is preceeded by a chronic periapical granuloma & stimulation of cell rests of malaseez present in the periodontal membrane.
Classification:-
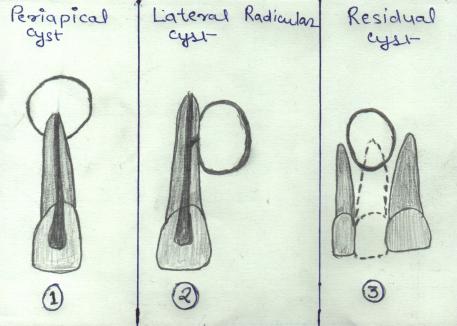
It is classified as follows—
1) Periapical Cyst:- These are the radicular cysts which are present at root apex.
2) Lateral Radicular Cyst:- These are the radicular cysts which are present at the opening of lateral accessory root canals of offending tooth.
3) Residual Cyst:- These are the radicular cysts which remains even after extraction of offending tooth.
19/03/2012 at 5:58 pm #15302drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 times19/03/2012 at 5:58 pm #15303drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 timesEtiology:-
A Radicular Cyst presupposes physical, chemical or bacterial injury resulting in death of pulp followed by stimulation of epithelial cell rests of malaseez which are present normally in periodontal ligament.Pathogenesis:-
Pathogenesis of Radicular Cyst is conveniently considered in 3 Phases, which are as follows
1) Phase of Inititiation,
2) Phase of Cyst Formation,
3) Phase of Cyst Enlargement
1) Phase of Initiation:- It is generally agreed that the epithelial lining of these cysts are derived from epithelial cell rests of malaseez in periodontal ligaments. However in some cases, epithelial lining may be derived from ,
a) Respiratory epithelium of Maxillary sinus when periapical lesion communicates with sinus wall.
b) Oral epithelium from fistulous tract.
c) Oral epithelium proliferating apically from periodontal pocket.
The mechanism of stimulation of epithelial cells to proliferate is not clear. It may be due to inflammation in periapical granuloma or some products of dead pulp may initiate the process & at same time it evokes an inflammatory reaction.
There is also evidence of local changes in supporting connective tissue which may be responsible for activating the cell rests of malaseez.
2) Phase of Cyst Formation:- It is a process by which cavity becomes lined by proliferating epithelium.
There are two Theories regarding it which are as follows:-
a) Most widely accepted theory suggests that initial reaction leading to cyst formation is a proliferation of epithelial rests in periapical area involved by granuloma. As this proliferation continues with the epithelial mass increasing in size by division of the cells on periphery corresponding to basal layer of surface epithelium. The cells of central portion of mass become separated further & further from nutrition in comparison with basal layer due to which they fail to obtain sufficient nutrition, they eventually degenerate, become necrotic & liqify. This creates an epithelium lined cavity filled with fluid.
b) The another theory suggest that a cyst may form through proliferation of epithelium to line a pre-existing cavity formed through focal necrosis & degeneration of connective tissue in periapical granuloma. But the finding of epithelium or epithelial proliferation near an area of necrosis is not common.
3) Phase of Cyst Enlargement:- Experimental work provided evidence that osmosis makes contribution to increase in size of cyst. Investigators found that fluids of Radicular cysts have Gamma Globulin level High by almost more than half to patient’s own serum. Plasma protein exudate & Hyaluronic acid as well as products of cell breakdown contribute to high osmotic pressure of cystic fluid on cyst walls which causes resorption of bone & enlargement of cyst.
Microbiology:-
Cyst may or may not be infected. Whenever infection is present Actinomyces organism have been isolated from radicular cyst commonly.
Microorganisms mainly found in root canal are 75% Gram +ve & 24% Gram –ve, among which Streptococci are predominant’ also other Gram +ve organisms like Staphylococci, Cornybacterium, yeast & others are found. Gram -ve organisms are Spirochetes, Nesseria, Bacteroids, fusobacterium, pseudomonas & others.
In Periapical lesions like Radicular cysts Obligate anaerobes are found.
Additionally in long standing cases of periapical pathology a- hemolytic & non hemolytic streptococci are found along with obligate anaerobes.
Medias used for Culture of Root Canal Materials – – –
– Brain Heart Infusion Broath with 0.1% Agar
– Trylicase Soy Broath with 0.1% Agar (TSA)
– Glucose Ascitis Broath
19/03/2012 at 6:00 pm #15304drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 timesClinical Features:-
A) Frequency:- It is most common cystic lesion of jaw comprising about approximately 52.3% of jaw cystic lesions
B) Age:- Large no. of cases are found in 4th & 5th decades of life after which there is gradual decline.
C) Sex:- It is more common in males comprising about 58% & in females comprising about 42%.
D) Race:-White patients are involved with a frequency of about twice that of Black patients.
E) Site:- It occurs with frequency of 60% in Maxilla. Though it may occur in all tooth bearing areas of both the jaws but preferably it occurs in maxillary anterior region. Upper lateral Incisors and Dense in Dente are usually the offending teeth. It occurs most commonly at apices of involved teeth. They may however be found at lateral accessory root canals.
Gross Features:-
Gross Specimen may be spheroidal or ovoid intact cystic masses, but often they are irregular & collapsed. The walls vary from extremely thin to a thickness of about 5mm. The inner surface may be smooth or corrugated yellow mural nodules of cholesterol may project into the cavity. The fluid contents are usually brown from breakdown of blood and when cholesterol crystals are present they impart a shimmering gold or straw colour.
Clinical Presentation:-
Smaller radicular cysts are usually symptomless and are discovered when IOPAs are taken with non-vital teeth.
Larger lesions shows slowly enlarging swelling. At first the enlargement is bony hard but as cyst increases in size, the covering bone becomes very thin, despite subperiosteal deposition & swelling exhibits springiness, only when cyst has become completely eroded, the bone will show fluctuation.
In Maxilla, there may be buccal and palatal enlargement Whereas in mandible it is usually labial or buccal & only rarely lingual.
Pain & infection are other clinical features of some radicular cysts. These cysts are painless unless infected. However, complain of pain is also observed in patient without any evidence of infection.
Occasionally, a sinus may lead from cyst cavity to the oral mucosa
Quite often there may be more than one radicular cyst. Scientists believe that there are cyst prone individuals who show particular susceptibility to develop radicular cysts.
Radicular cysts arising from deciduous tooth are very rare.Deciduous tooth which had been treated endodontically with materials containing Formecresol which in combination with tissue protein is antigenic & may elicit a humoral or cell-mediated response like rapid buccal expansion of cyst.
On rare occasion, there may be occurrence of parasthesia or there may be pathologic fracture of jaw bone take place.
Radiographic Features:-
Intra Oral Peri Apical Radiographs i.e. IOPAs are common radiographs which are used as diagnostic aid from radiological point of view.Radiographically , Radicular Cysts are round or ovoid radiolucent areas surrounded by a narrow radio-opaque margin, which extends from Lamina Dura of involved tooth. In infected or rapidly enlarging cysts, radio-opaque margins may not be seen. Root resorption is rare but may occur.
It is often difficult to differentiate radiologically between radicular cysts & apical granulomas.
Radiologic presentation of Radicular Cyst is given in detail as follows —
Periphery & Shape— Periphery usually have a well defined cortical border. If Cyst is secondarily infected, the inflammatory reaction of surrounding bone may result in loss of this cortex or alteration of cortex into more sclerotic border. The outline of radicular cyst usually is curved or circular unless it is influenced by surrounding structures such as cortical boundaries.
Internal structure— in most cases, internal structure of radicular cyst is radiolucent. Occasionally, dystrophic calcification may develop in long standing cysts appearing as sparsely distributed, small particulate radio-opacities.
Effects on surrounding structures— If a radicular cyst is large, displacement and resorption of roots of adjacent teeth may occur. The resorption pattern may have a curved outline. In rare cases, the cyst may resorb the roots of related non-vital teeth. The cyst may invaginate the antrum, but there should be evidence of a cortical boundary between contents of cyst and internal structure of antrum. The outer cortical plates of maxilla and mandible may expand in a curved or circular shape. Cyst may displace the mandibular alveolar nerve canal in an inferior direction.
19/03/2012 at 6:01 pm #15305drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 timesTreatment:-
1)Endodontic Treatment:-
Peripheral lesions including radicular cysts are eliminated by body once the causative agents are removed. Majority of radicular cysts can undergo resolutions following Root Canal Treatment & don’t require surgical intervenation. It is suggested that insertion of file or other root canal instrument beyond the apical foramen (for 1-2mm) produces transitory acute inflammation which may destroy epithelial lining of radicular cyst & convert it in to granuloma. Thus, leading to its resolutions.
2) Surgical Treatment:-
a) Enucleation- The affected tooth is extracted or preserved by root canal treatment with apicocetomy. A mucoperiosteal flap over cyst is raised & a window is opened in the bone to give adequate access. The cyst is carefully seperated from its bony wall. The entire cyst is removed intact. the edges of bony cavity are smoothened off, free bleeding is controlled and cavity is irrigated to remove debris. Mucoperiosteal flap is replaced back and sutured in place.
b) Marsupialisation- The cyst is opened essentially as for enucleation but the epithelial lining is sutured to mucous membrane at margins of opening. Yhe aim is to produce a self clensing cavity, which becomes an invagination of oral tissues. The cavity is initially packed with ribbon gauze & after margins are healed a plug or extension of denture is made to close the openings. The cavity usually closes by regrowth of surrounding tissues & restoration of normal contour of that part. However, there are always chances of closing the orifice & reformation of cyst. The main application is for temporary decompression of exceptionally large cyst where fracture of jaw is a risk factor. When enough new bone is formed, cyst can be enucleated.Prognosis:-
Prognosis depends on particular tooth, the extent of bone destroyed & accessibility for treatment.
Expected Complications:-
1) Carcinomatous/Neoplastic Changes:-
Squamous Cell Carcinoma or Epidermoid Carcinoma may occasionally arise from epithelial lining of Radicular Cyst.
2) Pathologic Jaw Fracture:-
If Cyst have completely eroded the bone specially if it is present in posterior region which is very rare in case of Radicular Cyst it may cause pathologic jaw bone fracture.
3) Secodary Infection:-
Cyst may get secondarily infected and create further complications.
21/03/2012 at 6:39 pm #15306 drsushant
OfflineRegistered On: 14/05/2011Topics: 253Replies: 276Has thanked: 0 timesBeen thanked: 0 times22/03/2012 at 6:42 am #15309
drsushant
OfflineRegistered On: 14/05/2011Topics: 253Replies: 276Has thanked: 0 timesBeen thanked: 0 times22/03/2012 at 6:42 am #15309drnpmhatre
OfflineRegistered On: 21/03/2012Topics: 0Replies: 1Has thanked: 0 timesBeen thanked: 0 timesabove material ( Posted by DrMithila) is from
http://radicularcyst.tripod.com
(this site was created by me in 2003)
22/03/2012 at 3:34 pm #15310smilesbyveeren@gmail.com
OfflineRegistered On: 31/03/2020Topics: 34Replies: 172Has thanked: 0 timesBeen thanked: 0 times22/03/2012 at 5:43 pm #15311drmithila
OfflineRegistered On: 14/05/2011Topics: 242Replies: 578Has thanked: 0 timesBeen thanked: 0 times -
AuthorPosts
- You must be logged in to reply to this topic.